
Breast pain or mastalgia is the most common complaint of most of the patients attending a Breast Clinic. Most of the time it is related to the aberration in the normal development and involution (ANDI), which in common language we call “Hormone-related”. The other causes are, peri-ductal mastitis, infection, trauma, chest wall related, lung-heart related, dyspepsia, and psychological. Most patients achieve good relief with placebo or minor treatment; however, a considerable number of patients may not be relieved with any treatment at all. In such patients, following excluding the psychological issues, we need to investigate further to find out the unusual cause. One important cause found in them is chest wall-related pain.
The chest wall comprises the muscles, bones, and pleura (membranous covering around the lungs). The problem with either of them may give rise to a pain not relieved with the routine medicines.

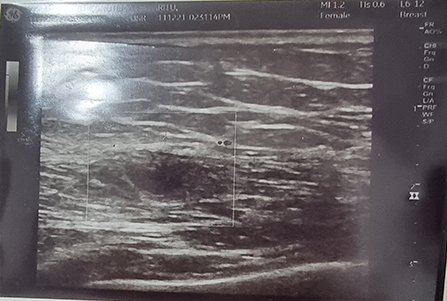
In our case, we had a 25-year multiparous female presenting with a vague swelling and continuous bothering pain in the upper inner quadrant of the right breast for the past few days, (Picture 1) following a minor impact by a child’s head. On examination, she had a vague swelling in her right breast in the upper-inner quadrant with slight tenderness. All the other findings were non-contributory. The ultrasound imaging showed bilateral prominent breast tissues (fibro adenosis – a finding commonly found in patients with ANDI) and a subtle intramuscular cystic lesion in the right pectoralis major muscle in the region of the pain (Picture 2).
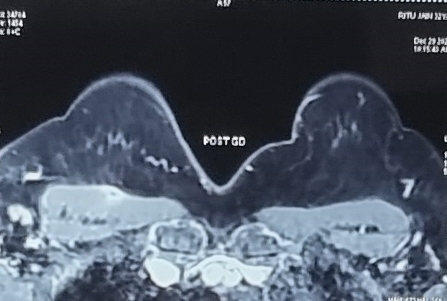
The initial probabilities were either fibroadenosis or trauma-induced muscular contusion. She was started on the usual treatment protocol for ANDI and traumatic pain. However, the patient returned within a week with the same complaint with no relief at all even after taking the painkillers and antibiotics. Founding her complaint to be genuine, she was investigated further with MR-MMG, A 4.9 X 5 mm cystic lesion with peripheral enhancement with peri-lesional edema was identified in right pectoralis major muscle suggesting intra-muscular cysticercosis (Picture 3).
The blood investigations revealed raised IgE levels, further supporting the diagnosis. Other than that, she was found to have osteomalacia with low vitamin D and calcium levels. She was managed with anti-helminthics like albendazole, and vitamin D and calcium supplements, following which she showed a dramatic response of >70% relief in her symptoms within 2 weeks.
Cysticercosis is a gut-worm infection caused by the larvae of the pork tapeworm, Taenia Solium. It is a major health concern worldwide especially in under-developed or developing countries. It is transmitted through the feco-oral route either due to ingesting the contaminated food or by consuming undercooked pork. Though the primary site of infection is the gut, the fertile eggs, also known as proglottids may retrogradely travel from the small intestine to the stomach, where due to gastric acid the embryos are released from the eggs, which then invade the gastric wall to enter the bloodstream and disseminate to any part of the body. The most common affected sites are the nervous system, subcutaneous tissues, muscles, eyes, and in rare cases heart and lungs. It can affect any age or sex.
The clinical features of cysticercosis depend on the location, cyst burden, and the associated inflammation. The course of the disease is waxing and waning. Fever is usually absent. There may be a history of trauma that triggers inflammation in an otherwise asymptomatic cyst. The clinical features vary from the asymptomatic case to those presenting with painful, tender swellings at the affected site due to cellular response initiated due to the leakage of the cystic fluid containing antigens following death or injury to the cyst. The diagnosis of intramuscular cysticercosis is often delayed or missed due to the non-specific clinical presentations. The three different clinical features described are the
1) Myalgic type- patient presents with vague muscular pain
2) Mass or pseudo-tumor like – patient presents with the tumor or nodule
3) Pseudo-hypertrophic type- patient presents with a vague muscular prominence. Our patient presented with myalgia and pseudo-hypertrophy.
Imaging evaluation is the key to identifying this entity. On high-resolution ultrasound, the cysticercosis usually appears as a cyst with an eccentric echogenic scolex. Other associated features could be perilesional edema or collection, or intra-cystic calcification. On MRI the lesion may appear as hyper-intense with well-defined and a hypointense intra-cystic eccentric nodule representing scolex. However, in smaller size lesions the typical findings may not be appreciable. In that situation, the clinical judgment based on the previous experiences helps in the diagnosis.
Albendazole and praziquantel are the two most used anti-cysticerci medicines. Steroids and anti-allergic are added to avoid any allergic reaction due to the massive release of the larval antigens.
Conclusion – Breast pain may be caused by various other conditions apart from the ANDI. Chest wall abnormality must be considered in patients not relieved with routine treatment. In patients with well-defined intra-muscular cystic lesions, especially in an endemic region, the possibility of intramuscular cysticercosis must be considered. Diagnosing this condition in a distressed patient is rewarding, since this is a completely curable condition.